

 Public Audit Act, 2004
Public Audit Act, 2004
R 385
National Health Act, 2003 (Act No. 61 of 2003)NoticesNational Health Insurance Policy towards Universal Health CoverageChapter 5 : National Health Insurance Coverage5.3 Service coverage |
| 102. | Service coverage refers to the extent to which a range of quality health services necessary to address the health needs of the population are covered. NHI will cover comprehensive health care services. |
| 103. | South Africans will be able to access personal health services covered by NHI closest to where they reside. The point of entry to accessing health services will be at the primary health care level with referrals to higher levels of care by providers at the PHC level. Properly delivered PHC could eliminate 21% to 38% of the burden of premature mortality and disability in children under-15 years of age, and 10% to 18% of the burden in adults. |
| 104. | These services will be delivered through certifiede and accreditedfhealth care providers located closest to the covered population to improve coverage from an allocative efficiency, affordability and sustainability perspective. PHC services will cover a catchment population that takes into account geographic, demographic and epidemiological profiles of the community. PHC services delivered by private providers will take into account the need to integrate providers into the delivery platform. There are several ways in which private providers could participate in offering PHC services including contracting–in or contracting-out.59 |
| 105. | At a PHC level, contracted-in services will be delivered by accredited providers normally practicing in the private sector but allocating a certain amount of time to render services in a public health facility such as a clinic. Contracted-out PHC healthcare services will be purchased from integrated teams of providers or networks structured as multidisciplinary practices of a wide range of health care professionals such as medical practitioners, dentists, nursing professionals, pharmacists, psychologists, audiologists, optometrists, physiotherapist, oral health practitioners and social workers amongst others. Those who practice as individual practitioners should be part of referral networks. |
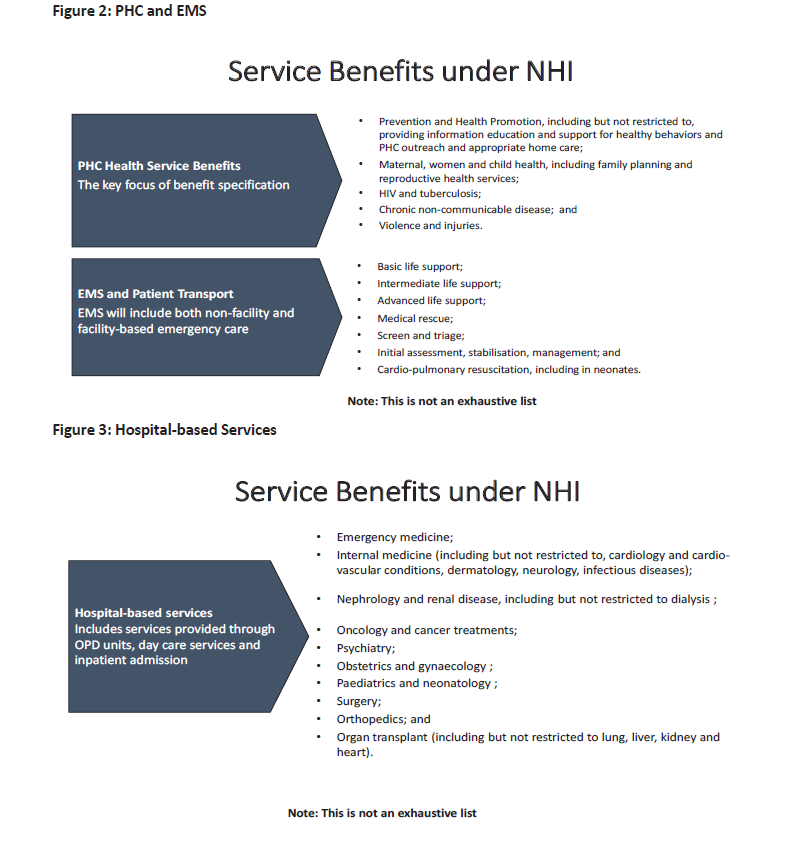
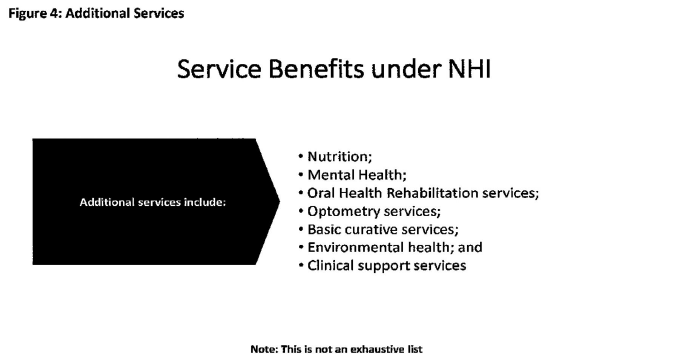
| 106. | The comprehensive set of personal health services will include a continuum of care from community outreach, PHC level based on the ideal clinic model, health promotion and prevention to other levels of curative, specialised, rehabilitative, palliative care, and acute emergency care. Health service benefits will be provided and described in terms of the types of services to be provided at each level of care with guidance on referral mechanisms. Services covered under NHI will also include access to pharmacies, and Emergency Medical Services. The comprehensive health services will cover (but not be limited to) the following: |
| 107. | NHI healthcare benefits will be portable throughout the country. Mobile healthcare services will be organised within a CUP. The contracting of accredited private providers will be prioritised with the aim of ameliorating geographical access challenges. Whilst assuring continuum of care communities, vulnerable groups (especially people with disabilities and the elderly) and those domiciled in rural settings may still experience limited access as a result of topography, and unaffordable transport costs. NHI will provide coverage for planned transportation in times of need and for the elderly and people with disabilities in rural and topographically inaccessible and rural localities. |
| 108. | Mental healthcare services will be fully integrated into PHC and higher levels of care with a view to increasing prevention, screening, care, treatment and rehabilitation including community mental health services. These services will include health promotion, and monitoring of related health outcomes delivered through registered councillors. There will be an appropriate referral system which also strengthens community mental health services. |
| 109. | Disability healthcare services will also be fully integrated into PHC with a view to increasing care, treatment and rehabilitation. Health infrastructure at all levels of care will provide for comprehensive rehabilitative services. These services will include provision of assistive devices, prosthesis and devices for assisting mobility. |
| 110. | NHI will cover comprehensive integrated occupational healthcare services that are responsive to diseases and injuries. The cornerstone of the delivery of occupational healthcare services will be based within the PHC model and integrated into the referral system to ensure the provision of treatment, care and support as well as rehabilitation assessments and services. |
| 111. | NHI will not cover non -personal health care compensation as this will still remain the responsibility of funds such as Compensation for Occupational Injuries and Diseases (COIDA) and Compensation Commissioner for Occupational Diseases in Mines and Works (ODMWA) – workplace will remain the responsibility of the employer and will not be funded through NHI but will be governed through the National Institute of Occupational and Communicable Diseases (NIOCD provisions). |
| 112. | The NHI Benefits Advisory Committee (BAC) will develop the comprehensive health care services for all levels of care (primary, secondary, tertiary and quaternary). The healthcare services will also include sexual and reproductive health, rare diseases and dread diseases. The NHI Benefits Advisory Committee supported by various committees will make evidence-based recommendations on what services, including surgical interventions are covered and the coverage for planned patient transport. |
| 113. | A process of priority setting60 and health technology assessment (HTA)61 will be used to inform the decision-making processes of the NHI Benefits Advisory Committee to determine the benefits to be covered. The range of services will be regularly reviewed using the best available evidence on cost-effectiveness, allocative, productive and technical efficiency62 and HTA. |
| 114. | The NHI healthcare services will not be based on a negative or positive list nor on a PMBs type of package. NHI priority setting will be through explicit guarantees63 using gate keeping at PHC level, a clearly articulated referral system, the use of clinical guidelines and protocols and HTA on the process of priority setting. |
| 115. | Detailed treatment guidelines, which are based on available evidence about the most cost-effective interventions, will be used to guide the delivery of the comprehensive health care services. Additional guidelines will be developed for interventions where such guidelines do not exist such as in surgical disciplines. All treatment guidelines will be routinely reviewed to take into account the assessment and appropriateness of new technologies. Efforts will be put into place to ensure that the general public is provided with the relevant information to support access and ensure empowerment regarding these guidelines. |
| 116. | Changes to the comprehensive health care service - including diagnostic tests covered under NHI will be informed by changes in the burden of disease, the demographic profile of the population and the evidence on cost-effectiveness and efficacy of health treatments, interventions and/or technology development locally and internationally. Changes and adjustments to the service benefits will be accompanied by a budget impact analysis. |
| 117. | An inventory of pharmaceutical, medical supplies and devices will be linked to the Essential Medicine List (EML) and will be updated on a regular basis by the EML Subcommittee of the NHI Benefits Advisory Committee. |
| 118. | Although the NHI healthcare service will be comprehensive and evidence-based, effort will be directed at ensuring that the covered services are medically necessary and have a positive impact on population health outcomes. |
| 119. | To ensure continuity of care, access to healthcare services covered will be portable. This will ensure that internal migrant populations visiting a different part of the country where they were not initially registered, can still access NHI healthcare services. Migrant populations must provide notice to the NHI Fund prior to embarking on the journey. |
______________________________________________
| e | Certified by Office of Health Standards Compliance (OHSC) |
| f | Accredited by the NHI Fund |
5.3.1 Expanding access to Hospital Services
5.3.2 Expanding access to pharmaceutical services
5.3.3 Expanding access to laboratory services
5.3.4 Expanding access to radiology services

